




Listen to Audio Version:
As a medical or healthcare provider, you are legally required to provide information to patients in their native or preferred language. Still, many practitioners see providing interpreters or translated documentation and forms as an inconvenience and added expense. If you are not prepared to provide services for these patients, you run the risk of liability for not following the law and being fined, as well as for the potential for malpractice suites because patient outcomes are compromised by misunderstandings. Misunderstandings that could have been avoided by using professional interpreters and translators.
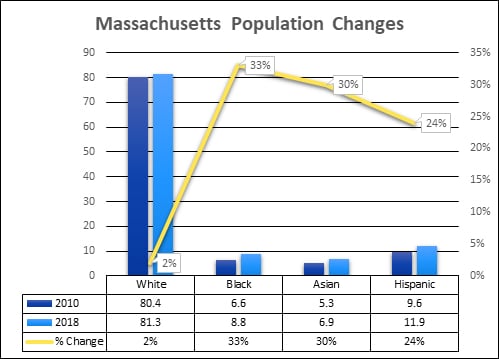
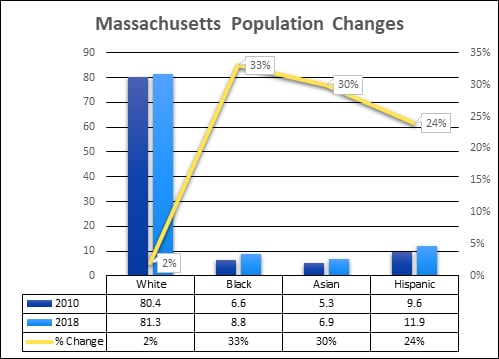
The Changing face of Massachusetts
Like the rest of the United States, the population in Massachusetts is changing and diversifying. The rate of culturally diverse residents is growing at a much quicker rate than that of white residents. This is a trend that is representative across the country as a whole.
- Nearly one in six Massachusetts residents is an immigrant, while one in seven residents is a native-born U.S. citizen with at least one immigrant parent.
- One in five workers in Massachusetts is an immigrant, together making up a vital part of the labor force in a range of industries.
- One in seven Massachusetts residents are native-born Americans with at least one immigrant parent.
 Avoiding Liability: Dangers and Difficulties in Patient Care
Avoiding Liability: Dangers and Difficulties in Patient Care
- 56% of hospitals offer interpretation and translation services, yet 97% of physicians see at least “some” limited English proficiency (LEP) patients
- Of 1,373 malpractice claims, at least 35 were linked to inadequate language access
- 46% of dental students do not feel prepared to treat LEP patients
- Half of surveyed physicians are unfamiliar with the legal requirements of working with interpreters
- Patients are unaware of how to file a complaint, so there is little recourse or follow-up
- Care providers can save millions of dollars each year by avoiding readmissions due to inadequate language services
- >40% of hospitalized LEP patients communicated without a professional interpreter
 Considerations When Caring for LEP Patients
Considerations When Caring for LEP Patients
Cultural & Family Issues - A patient traveled from the Middle East for a consultation regarding treatment of his advanced lung cancer. The doctor spoke through an Arabic interpreter and it appeared that interpretation was going very well, yet the emotional reactions seemed mild. A resident who spoke Arabic was at the meeting. When the patient left, the resident informed the physician that the interpreter did not tell the patient that he had cancer, he instead told him he had an infection and was going to get antibiotics, and everything was going to be fine. The resident explained that because the interpreter was of a lower social class than the patient, it was inconceivable for him to deliver the kind of news that was discussed in the meeting. (1)
Medicine efficiency - According to a recent study, today's medical school students appear to be getting the message that language-access issues aren't important and that they will be easily forgiven for a lax approach. The study concluded the problem stems from "a learning environment and organizational culture that value efficiency over effective communication."(2)
Misunderstandings & Ethics - A 9-year-old Vietnamese girl was rushed to the ER with what appeared to be the stomach flu. Her parents spoke no English, and no interpreters were used. The doctor prescribed a medication that isn't usually recommended for children, and hospital staff communicated in English with the girl and her 16-year-brother. The family was sent home with written instructions — also in English — to return to the hospital immediately if the girl experienced side effects. The girl had an adverse reaction to the drug, suffered a heart attack and died. This resulted in the physician and hospital settling a malpractice claim for $200,000. (2)
Additional Pain, Anxiety and Fear - An immigrant was given political asylum in the U.S. after living in Congo. He spoke limited English and feared the language barrier would make it difficult for him to seek treatment for his chronic stomach pain. When he sought treatment at a hospital in Washington, D.C. no interpreter was available, so he and the doctor struggled to communicate. "I asked him to use simple words, but that was hard for the doctor." (2)
Undocumented Immigrants - Clinicians occasionally find themselves confronting the phenomenon of potentially forcing “medical repatriation” of an immigrant patient when they lack means of financing the care. Undocumented immigration status preempts most of the usually available ways by which low-wage workers might secure insurance, either through private purchase or the provision of Medicaid. Thus, the health care institution seeks to discharge the patient to the only place that will accept him, the country of his birth. (3)
Untrained Interpreters - Research indicates that without trained interpreters, patient satisfaction and outcomes can plummet. A 2016 review of palliative care services concluded that patients who struggle with English don't adequately grasp their diagnoses without professional interpreters, and also had more pain and anxiety. (2)
Technology Issues - Technology for language services is improving and can be used to help address language barriers — but it is not always accurate. For example, in some British medical contexts, having seizures is sometimes referred to as "fitting" — as in, "having a fit." But a Swahili language app translated the English "Your child is fitting" to "Your child is dead" in Swahili. (2)
Services Unavailable - Often, some types of specialty services aren’t available in language. When a Spanish speaking patient was being treated for her breast cancer, she could not find a Spanish-speaking psychologist to help her understand how the chemo worked. And there was no Spanish-capable pain manager to assist with making her comfortable during treatment. (2)
(1)http://theoncologist.alphamedpress.org/content/13/5/586.full
(2) https://www.npr.org/sections/health-shots/2018/08/15/638913165/with-scarce-access-to-medical-interpreters-immigrant-patients-struggle-to-unders
(3) https://journalofethics.ama-assn.org/sites/journalofethics.ama-assn.org/files/2018-06/joe-1703.pdf page 222
Take Your Practice/Clinic/Hospital to the Next Level
By moving your localization process along the Localization Maturity Model (LMM) toward “Transparent” you improve efficiency, save time, save money and improve patient outcomes and experiences.
- Reactive – Responses to demands for multilingual communications and support is ad hoc and has an undefined process. Key characteristics of this stage are – no process, no team, minimal experience, unclear roles and responsibilities, no automation and heavy reliance on outside resources.
- Repeatable – This is a phase of discovery where basic project management processes start to form to track cost, scheduling and functionality. Key characteristics of this stage are – dedicated managers and clear roles, a repeatable process, some automation, integration of LSP services and a formal process of communication.
- Managed – In this stage multilingual communications becomes centralized and common problems are recognized and solved. The focus in this stage is toward optimization of execution and automation. Key characteristics of this stage are – dedicated team, metrics are well defined and tracked, more use of LSP services, increased use of language technology and more complex workflows to meet language service needs.
- Optimized – Quality and control are more closely observed and measured. External partners are managed more closely, and technology becomes more important in the process to decrease time and costs. Key characteristics of this stage are – a more scientific approach, translation management plan is implemented and utilized, QA is tracked, partnerships become more meaningful, metrics are monitored and integrated with organizational metrics.
- Transparent – In the highest stage of the LMM, localization is internalized as an integral part of the organization’s model and process. Focus is on continuous improvements and management. Key characteristics of this stage are – process is organization-wide, available to all, and part of overall organizational strategy.
You can avoid liability and improve efficiency and outcomes by working with an experienced multilingual communications company that has the skills to provide quality services as well as advise your organization or practice on how to move forward along the LMM. Rapport International has been providing high quality professional language services for more than 30 years. We value people-first communications because you don’t just need to pick the right language, you need to connect with your patients through clear communications. Contact us today to hear more about our services and discuss how we can help you do better.

Have questions
or need advice?
Sign up for a FREE 30-minute consultation with an expert.


Popular Posts
Popular industry news, interviews, technologies, and resources.







.png)